Jing-Sheng Zhao1,
Yuan-Liang Wei2,
Xin-Wei Lin1,
Hong Liu3,
Xue-Qing Xiao4,
Jun Yang1,
Wei-Guo Yi5 ![]() ,
Xiang-Nan Li6
,
Xiang-Nan Li6 ![]() ,
Dan Hao7
,
Dan Hao7
For correspondence:- Wei-Guo Yi Email: weiguoyipla@sina.com
Received: 17 August 2015 Accepted: 21 December 2015 Published: 28 February 2016
Citation: Zhao J, Wei Y, Lin X, Liu H, Xiao X, Yang J, et al. Effects of kangshen oral liquid on gentamicin-induced acute kidney injury in rats. Trop J Pharm Res 2016; 15(2):355-361 doi: 10.4314/tjpr.v15i2.19
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To investigate the effects of Kangshen oral liquid (KSOL) on gentamicin sulfate (GS)-induced acute kidney injury (AKI) in rats.
Methods: The rats were randomly divided into seven groups and treated with normal saline (NS), GS, furosemide, uremic clearance granule, or one of three different doses of KSOL. Several AKI-related indices were monitored, including renal index (RI), urine protein (UP) level, B-N-acetyl-glucosaminidase (NAG) activity in the urine, serum creatinine (SCr) level, blood urea nitrogen (BUN) level in the serum, malondialdehyde (MDA) level, and superoxide dismutase (SOD) activity in the kidney tissue. Histopathological changes in the kidney tissue of each group were monitored using light microscopy.
Results: After treatment with KSOL (20, 10, or 5 mL/kg), the RI, activity of NAG and levels of UP, SCr, BUN, and MDA were significantly decreased by 6.66 - 41.47 %, and the activity of SOD was significantly increased by 15.85 - 20.27 %, compared with the GS group (p < 0.05 or 0.01). The histopathological studies showed that KSOL notably improved GS-induced atrophy of the glomeruli, lymphocytic infiltration in the interstitium of the cortex, protein deposits in the collecting tubules, and hyperemia of the renal interstitium.
Conclusion: KSOL improves GS-induced AKI at biochemical and histopathological levels, and thus has a potential to be developed into a therapeutic drug for AKI.
Introduction
Acute kidney injury (AKI) is a common and important diagnostic and therapeutic challenge for clinicians [1]. It is characterized by a rapid decrease of renal excretory function and the accumulation of products of nitrogen metabolism such as creatinine, urea, and other waste products. Because the AKI definition emphasizes the filtration function of the kidney, it can be easily and routinely diagnosed by analyzing the serum creatinine (SCr) and urea concentrations [2,3].
The use of vasopressors and conditions such as diabetes mellitus, chronic renal disease, and sepsis are some triggers for AKI, while hypovolemia, creatinine on admission, and high severity scores are clinical indicators of the condition [4-6]. The mortality of AKI patients is 60 - 70 % [7,8]. About 20 - 40 % of AKI patients die in the hospital, and the mortality rates are even higher in patients who suffer from severe AKI [9,10]. Currently, specific therapies have not been developed to prevent or cure AKI. Patients who survive AKI often suffer from chronic kidney disease or end-stage renal disease [11,12]. Therefore, it is critical to develop new, safe and effective drugs to prevent or treat AKI.
Based on the knowledge of the compatibility and characteristics of traditional Chinese medicines (TCMs), Kangshen oral liquid (KSOL), which consists of: Ginseng radix et rhizoma (150 g), Astragali radix (200 g), Atractylodis Macrocephalae rhizoma (150 g), Poria (200 g), Epimedii folium (150 g), Dioscoreae rhizoma (150 g), Pheretima (100 g), Carthami flos (200 g), Rosae Laevigatae fructus (200 g), Euryales semen (100 g), and Glycyrrhizae radix et rhizoma (40 g), was developed by Wei-Guo Yi, Xiang-Nan Li and their team to help patients with AKI. The aim of this study was to investigate the effects of KSOL on gentamicin sulfate (GS)-treated AKI in rats by observing the histopathological changes of kidney tissue and determining AKI-related indices, such as the renal index (RI), the urine protein (UP) level, the B-N-acetyl-glucosaminidase (NAG) activity in the urine, the serum creatinine (SCr) and blood urea nitrogen (BUN) levels in the serum, as well as the malondialdehyde (MDA) level and superoxide dismutase (SOD) activity in the kidney tissue.
Methods
Plant materials
Ginseng radix et rhizoma, Astragali radix, Atractylodis Macrocephalae rhizoma, Poria, Epimedii folium, Dioscoreae rhizoma, Pheretima, Carthami flos, Rosae Laevigatae fructus, Euryales semen, and Glycyrrhizae radix et rhizoma were purchased from Beijing TongRenTang Co., Ltd and identified by Wei-Guo Yi, who work in Department of Medicine, the 152nd Central Hospital of PLA (Pingdingshan, China). Eleven voucher specimens for each crude drug (voucher nos. 152CHPLA2009010 - 152CHPLA2009020) were stored in Dalian Medical University (Liaoning, China) for future reference.
Chemicals and reagents
Uremic clearance granule (UCG) was purchased from Inner Mongolia Shankangchen Pharmaceutical Industry (batch no. 20110114). Furosemide was obtained from Tianjin Lisheng Pharmaceutical Co., Ltd (batch no. 1101008). Normal saline (NS) was provided by Henan Tailing Pharmaceutical Co., Ltd., (batch no. 11082465). GS was manufactured by Henan Furen Huaiqingtang Pharmaceutical Co., Ltd., (batch no. 1108301). Formalin was purchased from Yantai Shuangshuang Chemical Co., Ltd., (batch no. 20110310). Acetic acid was obtained from Tianjin Hengxing Chemical Reagent Co., Ltd., (batch no. 20110114). The SCr assay kit (batch no. 20111223), urea assay kit (batch no. 20111223), UP test kit (batch no. 20120109), NAG assay kit (batch no. 20111201B), SOD assay kit (batch no. 20120105), and MDA assay kit (batch no. 20111227) were purchased from Nanjing Jiancheng Bioengineering Institute, China.
Animals
Adult Wistar rats (200 ± 20 g) were obtained from Hebei Experimental Animal Center and housed in metabolic cages (25 °C, 12 h light/dark cycle). All animals received water and food ad libitum. Animal treatments were conducted in strict accordance with the ethical guidelines of the National Institutes of Health Guide for the Care and Use of Laboratory Animals [13]. Experiments were carried out with the approval of the ethics committee of the 152nd Central Hospital of PLA (protocol no. 2009092632).
Preparation of KSOL
KSOL was provided by the 152nd Central Hospital of PLA’s manufacturing laboratory (batch no. 20110425). KSOL was prepared as follows. According to the ratio described above, 11 kinds of TCMs were finely ground and boiled thrice with water for 40 min. The combined decoction filtrate was concentrated under reduced pressure by rotary evaporators to reach a relative density of 1.15 - 1.30 at 80 °C, and then the concentrate was diluted with ethanol to obtain a 60 % ethanol solution. The resulting solution was incubated standing at room temperature for 24 h. After filtration, the ethanol solution was condensed under reduced pressure by rotary evaporators to remove the alcohol, and simple syrup was added into the solution. The above solution was diluted to 1000 mL (pH = 5.0 - 7.0) with water, and then the diluted solution was filtrated and sterilized to produce KSOL.
Grouping, modeling, and treating
Eighty-four Wistar rats were randomly divided into seven groups (n = 12) to receive one of seven treatments: NS, GS, furosemide, UCG, or one of the three different doses of KSOL. Rats treated with GS, furosemide, UCG, or KSOL were first injected intraperitoneally with 140 mg GS/kg at 9:00 a.m. once a day for 7 days to establish the AKI model. Meanwhile at 6 p.m. each day, rats in the GS, furosemide, or UCG groups were separately administered orally with NS, 6.6 mg furosemide/kg, or 4.2 g UCG/kg, and rats in the KSOL groups were administered orally with high (20 mL/kg), middle (10 mL/kg), or low (5 mL/kg) doses of KSOL, respectively. Rats in the NS group were injected intraperitoneally with NS at 9:00 a.m. and administered orally with NS at 6 p.m. once a day for 7 days. All drugs were dissolved in NS or diluted with NS to obtain different concentrations such that the rats received an intragastric volume of 20 mL/kg.
After 1 h of drug treatment on 7th day, rats were transferred to metabolic cages, and the urine excreted by the rats was collected over 24 h and used to determine the NAG activity and UP level. Orbital blood was gathered on the 8th day and centrifuged at 3000 r/min for 10 min at 4 °C to obtain serum, which was used to determine the SCr and BUN levels. Subsequently, the rats were sacrificed by decapitation, and their kidneys were removed and washed with NS, blotted with a piece of filter paper and weighed. The right kidney was homogenized and centrifuged at 3000 r/min for 10 min at 4 °C to obtain the supernatant, which was used to analyze the SOD activity and MDA level. The left kidneys were isolated for histopathological investigation. RI was calculated as in Eq 1.
RI (%) = (A/B)100 ……………………………. (1)
where A and B stand for the weight of the renal parenchyma and the body weight, respectively.
Biochemical determinations
The levels of UP, SCr, BUN, MDA, and the activities of NAG and SOD were determined using the corresponding kits according to the manufacturer’s instructions for each [14-16]. After reactions were completed, absorbance was determined for all samples using a UV-visible spectrophotometer (Unico Shanghai Instrument Co. Ltd., China) or a 680Microplate Reader (Bio-Rad, USA).
The detection wavelengths for UP, SCr, BUN, MDA, NAG, and SOD were set at 595, 510, 640, 640, 450, and 560 nm, respectively. The absorbance for these indices was used to calculate the level or activity according to the corresponding standard curves.
Histopathological studies
Tissue fragments were taken from the left kidney tissue from representative rats in each group and fixed in 10 % formalin. The fixed kidney tissue was washed six times with PBS, dehydrated in ethanol, and embedded in paraffin. The embedded tissue fragment was sliced at 3 μm, and the slices were stained with hematoxylin and eosin (H&E) for light microscopy.
Statistical analysis
All data are presented as mean ± standard deviation (SD) and were analyzed by one-way ANOVA using SPSS 19.0 (IBM SPSS Statistics, USA). Differences were considered to be statistically significant at p < 0.05.
Results
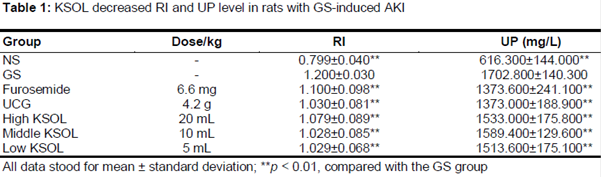
KSOL decreased RI and UP level in rats with GS-induced AKI
As shown in , the RI and UP level in the GS group were increased significantly, compared with the NS group (p < 0.01), indicating that the AKI model was successfully established with GS treatment. Furthermore, these increases were reversed by treatment with furosemide or UCG, suggesting that the injuries could be reversed successfully with known treatments. After treatment with KSOL (20, 10, or 5 mL/kg), the RI and UP level were decreased significantly relative to the GS group (p < 0.01), suggesting that the KSOL offered an improvement to AKI injury in this model.
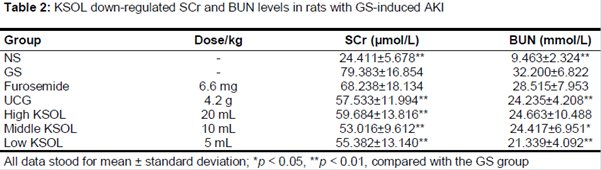
KSOL down-regulated SCr and BUN levels in rats with GS-induced AKI
As shown in , the SCr and BUN levels in the GS group were increased significantly, compared with the NS group (p < 0.01), indicating that the AKI model had been successfully established. After treatment with UCG or KSOL (20, 10, or 5 mL/kg), the SCr level was decreased significantly, compared with the GS group (p < 0.01). After treatment with UCG or KSOL (10 or 5 mL/kg), the BUN level was decreased significantly relative to the GS group (p < 0.05 or 0.01).
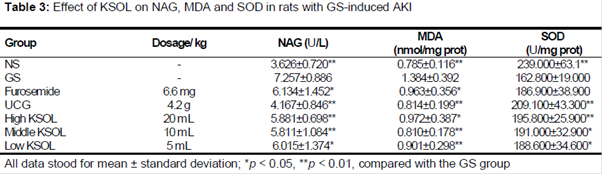
Effect of KSOL on MDA level, NAG activity and SOD activity in rats with GS-induced AKI
As depicted in , MDA level and NAG activity in GS group were increased significantly, and the SOD activity was reduced significantly, compared with the NS group (p < 0.01). These data indicated that the AKI model was successfully established. After treatment with furosemide, UCG, or KSOL (20, 10, or 5 mL/kg), the MDA level and NAG activity were reduced significantly, compared with the GS group (p < 0.05 or 0.01). After treatment with UCG or KSOL (20, 10, or 5 mL/kg), the SOD activity was increased significantly, compared with the GS group (p < 0.05 or 0.01).
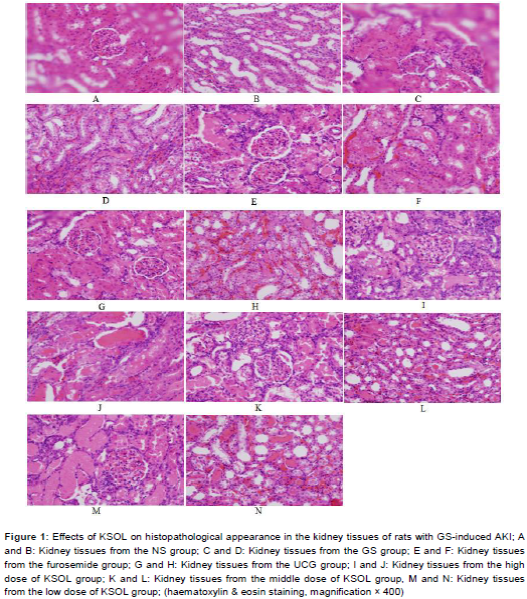
Effect of KSOL on histopathological characteristics of kidney tissue of rats with GS-induced AKI
In the NS group, glomeruli, renal tubules, and collecting tubules were normal (A and B). In the GS group, the glomeruli were atrophied, and the epithelial cells of the tubules had extreme edema, which resulted in stenosis of the lumens. There was severe lymphocytic infiltration in the interstitium of the cortex. Significant protein deposits were observed in the collecting tubules, and the renal interstitium was hyperemic (C and D).
In the furosemide groups, the glomeruli were normal, but the epithelial cells of tubules exhibited edema. Protein deposits were observed in the renal tubules and severe lymphocytic infiltration was observed in the interstitium of the cortex. Protein deposits had accumulated in the collecting tubules, and the renal interstitium was hyperemic (E and F). In the UCG group, the histological sections were similar to those in the furosemide group, except that the renal interstitium exhibited extreme hyperemia (G and H).
In the high-dose KSOL group, the histological sections were similar to those from the furosemide group (I and J). In the middle dose of KSOL group, the histological sections were similar to those from the furosemide group, except that there were some protein deposits in the renal tubules and slight lymphocytic infiltration in the interstitium of the cortex (K and L). In the low dose of KSOL group, the histopathological characteristics were similar to those observed in the UCG group (M and N).
Discussion
Administration of GS is considered an acceptable model to induce AKI in rats. Upon GS administration, several physiological markers are used to measure the severity of AKI, including RI and UP levels, NAG activity in urine, serum SCr BUN levels, and renal MDA level; all of these increased under conditions of AKI. Additionally, SOD activity is decreased in rat kidney with AKI [17-19]. We observed all of these physiological changes in our AKI model. Moreover, many histopathological characteristics, including atrophy of the glomeruli, lymphocytic infiltration in the interstitium of the cortex, protein deposits in the collecting tubules, and hyperemia of the renal interstitium, can be observed in rat kidney with GS-induced AKI [17-19].
In the present study, we investigated the effect of KSOL on GS-induced AKI in rats by measuring these various AKI-related indices and histopathological changes. We confirmed that GS can induce all of these changes in this rat model of AKI. Furosemide and UCG each offer a protective effect on the kidney, and thus served as positive control treatments [20,21].
Several physiological indices can be used to evaluate the overall health of the kidney. RI is a simple index to reflect edema of the kidney, and an increase in RI indicates that edema of the kidney has occurred [22]. UP can reflect filtration function of the kidney, where kidney damage is reflected by an increase in UP level [19]. Although glomerular filtration rate (GFR) is the best overall index of renal function in health and disease [23], it is difficult to measure in clinical practice. Therefore, most clinicians estimate the GFR based on the SCr level [24]. Renal parenchymal injury can lead to an increase in BUN level [19].
NAG, a lysosomal enzyme whose molecular weight does not permit filtration through glomeruli, exists in the proximal tubular cells. An increase in NAG activity in the urine indicates that kidney dysfunction has occurred [25]. MDA level can assess lipid peroxidation, which can induce tissue damage through oxygen-free radicals [26]. An increase in MDA level in kidney tissue indicates that lipid peroxidation has occurred. SOD is an essential defense against the damage of superoxide [27].
The mechanism of GS-induced nephrotoxicity seems to be a result of destructive reactive oxygen species, which can participate in kidney injury [19]. Thus, increase in SOD activity can accelerate recovery from AKI. In this study, KSOL exhibited a protective effect on GS-induced AKI in rats at the biochemical level by increasing the activity of SOD and reducing the RI, activity of NAG, and levels of UP, SCr, BUN and MDA.
Moreover, our results show that KSOL improved GS-induced histopathological characteristics in the kidney tissue of rats with AKI, including atrophy of the glomeruli, lymphocytic infiltration in the interstitium of the cortex, protein deposits in the collecting tubules, and hyperemia of the renal interstitium.
Conclusion
KSOL has a protective effect on GS-induced AKI in rats by increasing the activity of SOD and decreasing RI, NAG activity, as well as levels of UP, SCr, BUN and MDA. KSOL also improves the histopathological profile of kidneys. Thus, KSOL is capable of preventing the toxic effects of GS on kidneys at biochemical and histopathological levels, and thus has a potential to be developed into a therapeutic treatment for AKI.
References
Archives


News Updates